COPD and Osteoporosis
This Special Study Component was designed to answer the question “Should COPD patients be routinely monitored for bone mineral density?”. It consists of four sections: Introduction; Literature Review; Critical Appraisal; Discussion and Conclusions. Parts of this assignment have been edited to remove patient-specific information. A full bibliography of sources is provided at the end. Click on figures and diagrams to enlarge them.
Please remember that this is merely a medical school assignment, and does not constitute medical advice.
Introduction
The Special Study Component allows students to choose a topic related to either the Patient Study or Community Placement and explore this in greater depth than the core medical curriculum otherwise allows. I became particularly interested when I came across a patient who had both chronic obstructive pulmonary disease (COPD) and osteoporosis; discussion with my colleagues revealed that many other patients with COPD also have osteoporosis.
In these patients, osteoporosis can lead to fracture, for example factured femurs, which cause great discomfort and restrict mobility even further than the level to which it is already restricted due to COPD. If osteoporosis could be detected when the first signs appear, then treatment could start earlier and, perhaps, distress such as that experienced by my patient could be avoided. This stimulated the idea of a potential link between the two conditions, and this occurred to me to be a potential basis for the Special Study Component.
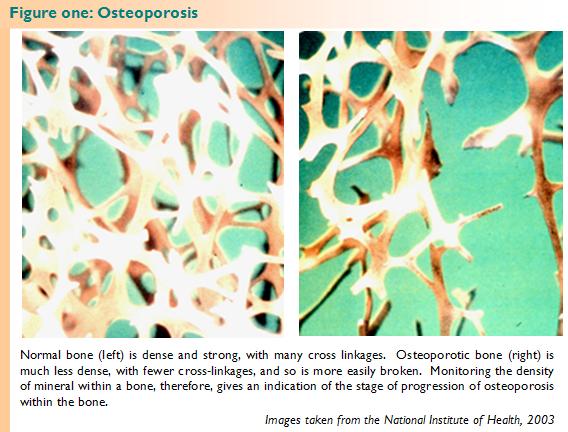
Osteoporosis is generally asymptomatic until it reaches a level of severity at which a bone is fractured, and so treatment often does not occur until the osteoporosis is quite severe. It occurred to me that bone density monitoring may be beneficial to a group in which osteoporosis incidence is particularly high, so that appropriate treatment can begin before any acute incident occurs. I therefore decided to write my SSC around the investigation of whether routine bone density monitoring would be beneficial for patients with COPD.
Through basing my SSC in this clinical grounding, I hope that my practical knowledge as a clinician will be increased through its completion, rather than treating it as a purely academic exercise.
Literature Review
In order to discuss whether routine bone mineral density monitoring (see figure one) would be an appropriate measure to help combat osteoporosis amongst chronic obstructive pulmonary disease (COPD) patients, it is first important to establish whether a link between the two diseases exists.
Biskobing (2002) in an extensive review, suggests that there is a higher rate of incidence of osteoporosis among patients with COPD than among the general population, and this, in turn, suggests that there exists a link between the two. The nature of this link, however, is unclear. Without discovering the nature of the link, it is impossible to say whether it is likely to affect a large proportion of the population of patients with COPD, and thus impossible to make recommendations as to which (if any) measures to detect osteoporosis are appropriate. It is therefore prudent to look at the causes of osteoporosis, and how these may be altered in patients with COPD.
Osteoporosis has a wide range of different causes, including smoking, low body mass index, corticosteroid use, and a lack of regular exercise (Biskobing, 2002). Biskobing investigates a number of risk factors for osteoporosis among COPD patients. Biskobing finds that smoking alone increases the risk of osteoporosis, and since the vast majority of COPD sufferers are, or have previously been, smokers, this increases their risk. The risk of osteoporosis is increased with decrease body mass index figures, and these are common amongst COPD patient. Corticosteroid use can lead to hypogonadism, a risk factor for osteoporosis, and also cause osteoporosis itself. Finally, the immobility conferred upon COPD patients by their breathing difficulties leads to Vitamin D deficiency since they tend to stay indoors, and decreased muscle strength, both of which are also risk factors for osteoporosis. Taking all of these factors into account, Biskobing recommends bone mineral density (BMD) monitoring for COPD patients.
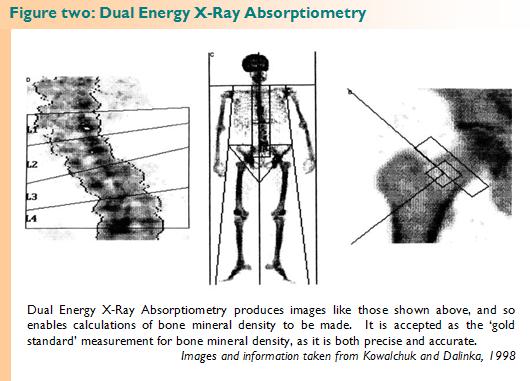
BMD monitoring can be most accurately achieved using dual energy X-ray absorptiometry (DEXA), although other methods can also be used in particular situations. DEXA is a completely non-invasive procedure which is generally acceptable to patients. It is also a quick procedure, and is essentially similar to administering a traditional plain-film radiograph. (Kowalchuk and Dalinka, 1998) More information on DEXA is shown in figure two.
I feel that it would be sensible to do further research into which factors are most important in the development of osteoporosis before making recommendations about BMD monitoring, since finding such information could help to identify groups which are at particular risk, thereby removing the need to screen all patients, thus avoiding the unnecessary use of resources, as well as inconvenience to individual patients.
Melton et al. (2004) conducted a retrospective population-based cohort study into the fracture risk following adult-onset asthma. Their definition of adult-onset asthma was wide enough to include a number of COPD patients within the population. The researchers used data from 226 patients over a number of years, including the medications supplied to them and the number of fractures each patient experienced.
They found that the fracture risk was increased mainly in those patients with COPD, and that this risk was directly influenced by the use of systemic corticosteroids. Those patients who used only topical corticosteroids were found to have no increased risk for osteoporosis.
This suggests that oral corticosteroids are possibly the most important factor, since only the COPD patients treated with these had a significantly higher risk of developing osteoporosis. Other patients with similar conditions not treated with corticosteroids apparently did not display the same level of increased risk.
A study investigating a link between corticosteroids and osteoporosis was conducted by Walsh et al. (2002). This team followed 117 patients using oral corticosteroids, and measured their BMD using X-ray absorptiometry. In this study, steps were taken to exclude patients who may have other factors which may lower their bone mineral density, such as those taking other drugs known to affect BMD.
Walsh et al. found that the use of these steroids is associated with an increased risk of bone fracture, but found only limited evidence to support the idea of a direct link between corticosteroid dose and the degree of osteoporosis experienced. They also found that there was an increased rate of fracture among patients taking corticosteroids than can be explained using BMD alone.
The lack of a direct relationship between dose and response would suggest that there is another factor in the administration of corticosteroids which could explain why there appears to be a link, but not a clear dose-response relationship. The increased rate of fracture over and above that which can be explained by BMD presents an interesting problem, although it would appear that this study is unusual in this finding. Since the study was relatively small, it could be that the data for risk of fracture was inaccurate as a population picture because several of the participants may have had a higher rate of accidents which caused fractures, or perhaps had accidents which fractured multiple bones. As none of the larger studies found a similar effect, it seems reasonable to dismiss it as an experimental error.
Dubois et al. (2002) conducted a study into the use of glucocorticoid treatment regiments and development of osteoporosis in COPD patients. The team recruited eighty-six white men with COPD and split them into four groups based on their glucocorticoid treatment history: A group who had received continuous treatment through a daily dose of at least 10mg, a group who had multiple courses whose cumulative total was more than 1000mg, a group who had multiple courses whose cumulative total was less than 1000mg, and a control group who had never received systemic glucocorticoids.
The outcome of the study was that those patients who received more than 1000mg of glucocorticoids over multiple courses to treat acute incidents were at a greatly increased risk of developing osteoporosis, with some eighty-two percent of patients within this group developing the condition. However, those who were administered small amounts glucocorticoids on a constant, on-going basis did not develop osteoporosis, despite having a cumulative dose of almost ten times that of the patients in the multiple dose group.
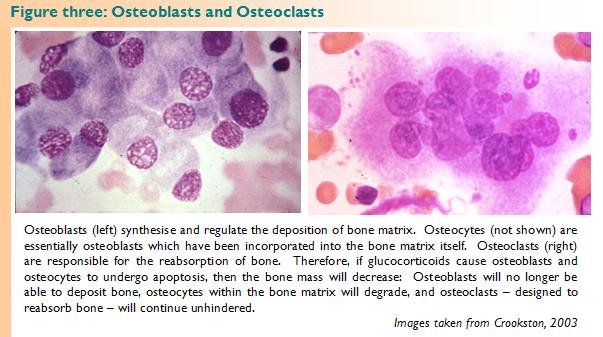
The group hypothesised that introduction of glucocorticoids induces apoptosis of osteoblasts and osteocytes, which leads to a reduction in bone formation and hence a loss of total bone mass (see figure three). This loss of bone mass occurs rapidly when the glucocorticoids are first administered, due to osteoclast-mediated bone reabsorption, which is probably the result of extended osteoclast life span. After approximately one year, the bone loss slows and plateaus. The researchers therefore theorise that those patients treated with glucocorticoids on an ongoing basis only have one drop in bone mass, at the beginning of their treatment, whereas those who receive glucocorticoid treatments on a more sporadic basis to treat acute incidents have a number of major drops in bone mass, leading to osteoporosis.
The group who had multiple doses amounting to less than 1000mg – that is, they had fewer doses than the other multiple dose group – had a lower risk of osteoporosis than those in the other multiple-dose group, but a higher risk than those in the continuous group. This is consistent with the hypothesis, since these patients would have experienced fewer introductions of the drug and so fewer drops in their bone mass, but more than those who were on the continuous drug provision.
This theory is supported by the evidence from Walsh et al. (2002) who were unable to find a direct dose-response relationship between the two factors. The total dose is of little relevance; but the manner of their administration, in particular whether the drug is supplied continuously or sporadically, is of crucial importance.
The work of Karadag et al. (2003) supports the hypothesis proposed by Dubois et al. (2002). In this study, twenty-eight clinically stable patients with moderate COPD were chosen. Of these patients, only fourteen had received any systemic corticosteroids, and none of these patients had received more than four short courses. When these patients’ BMDs were measured and compared with those of a control group with normal pulmonary function, there was found to be no significant difference. This clearly supports the Dubois et al. (2002) hypothesis, which states that it is corticosteroid treatment which causes osteoporosis in COPD patients.
However, the work of Sin et al. (2003) finds data that is contradictory to the Dubois et al. (2002) hypothesis. They analysed data from almost 10,000 Caucasian citizens of the United States, thirteen percent of who were found to have some degree of airflow obstruction upon spirometry testing.
The researchers discovered that those patients with greater airflow obstruction showed a greater risk of developing osteoporosis. This trend was found to be ‘independent of age, body mass index, and medications used – including recent use of corticosteroids’. This suggests that the risk of osteoporosis is increased due to some inherent factor related to the breathing difficulty itself. As a result of this, Sin et al. (2003) suggest that BMD monitoring should be standard for all patients with COPD. However given that only one percent of their study participants were taking oral corticosteroids, and that it seems unlikely that the researchers would even have been looking for the right kind of trend, it is, perhaps, not surprising that they do not find one.
Taking the articles I have reviewed as a whole, it would appear that vast majority of patients displaying osteoporosis have previously been treated with corticosteroids. Those not treated with corticosteroids do not show osteoporosis. I suggest, therefore, that it is corticosteroids which cause osteoporosis in COPD patients, and so BMD monitoring for all patients with COPD is not the best solution to the problem, since BMD monitoring could cause both unnecessary distress and inconvenience to some COPD patients who, in fact, were not at any increased risk for osteoporosis. Furthermore, the use of healthcare resources to undertake this BMD monitoring could financially disadvantage more useful areas of patient care.
However, given the apparent increased risk to patients treated with corticosteroids shown by these papers, and considering the acceptability to the patient of DEXA, I recommend that patients treated with corticosteroids should be monitored for BMD.
Critical Appraisal
In this section, I intend to critically appraise two of the articles used in the Literature Review. First, I shall examine Dubois et al, 2002, and second, I shall appraise Sin et al, 2003.
I have chosen to appraise Dubois et al. (2002) because this is the paper whose hypothesis almost all of the data from the other studies appears to fit. It therefore seems prudent to examine in detail the experimental methods used, to see whether the hypothesis proposed is supported by the data put forward in the study.
Dubois et al. (2002) attempted to compare bone mineral density outcomes of patients who received continuous oral systemic glucocorticoids with those who received mutiple courses, either orally or intravenously. This seems to be a rather irregular comparison to make, since one would expect the team to compare like with like – that is, I would expect them to compare continuous oral courses with multiple oral courses, and not complicate the situation by also allowing multiple IV courses into the study. The reasons for this decision are not made clear in the paper itself.
Eighty-six men with documented COPD for at least five years were included in the study, having been recruited from all COPD patients in a named group of hospitals. These men were then split into categories according to their complete glucocorticoid treatment history. A control group of thirty-seven patients with COPD who had never been treated with glucocorticoids was also included.
Because of the small size of the study, splitting the patients into four groups left each group with a very small number of participants: Only ten in the case of the continuously adminstered glucocorticoid group. Furthermore, there were some compounding problems in assigning groups, in that some of the participants in the continuous group had also received some additional short courses of glucocorticoid, which would otherwise put them in a separate category. These seems an unfortunate decision to take, because it means that each small group does not contain subjects which fit entirely within that category.
Bone mineral density was measure using DEXA (see figure two, page 6). However, as a retrospective study, it was impossible for the team to take readings of BMD before the treatment commenced, and so they are not able to compare before and after treatment. This makes it difficult, particularly given that the sample sizes are so small, to rule out the possibility that any osteoporosis detected at the end of the study was not a mere progression of disease that may have been present before the treatment was commenced.
Dubois et al. found that the majority (82%) of the subjects in the group which received multiple doses of glucocorticoids amounting to a cumulative total of over 1000mg had osteoporosis. This was a much higher figure than for any of the other groups. Statistical testing showed that the only relationship with osteoporosis was with glucocorticoid adminsitration, and that no other variable on which data had been collected formed a relationship.
The team went on to conclude that exposure to multiple courses of glucocorticoids was a large risk factor for osteoporosis, and suggested that those patients receiving such courses should have their BMD checked in an early phase of the management of the disease.
Given the size of the study, and the fact that it was impossible for the researchers to compare before-and-after figures, I think that their conclusion probably extends further than the data truly allows. With such a small study population, I think that questions are raised over whether the group in question, consisting of just eleven patients, is truly representative of all patients taking multiple courses of glucocorticoids. It is also impossible for the team to establish conclusively that it is the glucocorticoids that have caused the osteoporosis. Therefore, in order to truly prove the hypothesis proposed, much more research needs to be done in this area. It is simply not possible to accept this hypothesis using only the data presented in the paper.
The second paper I have chosen to appraise Sin et al (2003) primarily because it was the single article from the literature review which did not appear to fit the hypothesis presented by Dubois et al. (2002), and by critically appraising the article I hope to be able to discover whether this disagreement could come about through an experimental artefact or error in the way the experiment was conducted.
Sin et al. (2003) have chosen to conduct this study because they felt there was little generalisable data about the potential link between osteoporosis and airflow obstruction in relation to patients with mild-to-moderate airflow obstruction. They hope that by providing a large study into this, they will be able to produce data which can be generalised for the population as a whole.
The team used data from the Third National Health and Nutrition Examination Survery (NHANES III), which was a survey with 20,000 participants in the USA, conducted between 1988 and 1994. The participants, chosen as a stratified sample of the population, were asked to complete a questionaire and undergo a comprehensive physical examination. From this very large data set, Sin et al. chose only the 9502 Caucasian participants of twenty years of age or above, who had valid body mass index and spirometry information. This seems a particularly unusual choice for the team to make, considering that they were trying to make the study generalisable to the population as a whole. In order to do this, it would seem to make more sense to use the data set from the whole stratified sample, rather than taking a subset of the population with particular physical characteristics. The team also fail to define what values for BMI and spirometry tests they have defined as ‘valid’. However, this method does remove many of the normal variations which may have hindered analysis of the data.
By using data from another study, Sin et al. clearly had no control over the way the measurements were taken for each individual, and so could not tailor them to be the most appropriate and accurate measurements for the trends they were looking for.
The data Sin et al. chose to use has some particularly concerning abnormalities. Firstly, they did not take a complete medical history from the participants, and only included medications taken by the participants within one month of the survey being undertaken. Therefore, a patient could have been taking medication for many years and have recently stopped, and this would not have been shown in the data. In order to estimate the physical activity of the participants, which would appear to be a particularly important factor when assessing airflow obstruction, the surveyors asked only two questions: ‘In the past month, did you walk a mile or more without stopping?’ and ‘In the past month, did you garden or work in the yard?’. Clearly, these questions do not provide a very good estimation of someone’s physical activity, not least since people without a garden or back yard would appear to do little physical activity by the latter measure, and those with mobility difficulties would appear to do little by the former measure.
However, measurements for bone mineral density were made using the standard dual-energy x-ray absorptiometry, and lung function tests were also satisfactorily completed to standards set by an independent body.
After statistical analysis of this clearly flawed data, Sin et al. concluded that ‘airflow obstruction, independent of age, body mass index, and medications… increased the risk of osteoporosis in a severity-dependent fashion’. Given that the team only looked at data on medications for one month prior to the study, it seems that this conclusion goes some way beyond the data which was supplied. For example, the hypothesis put forward by Dubois et al. (2003) suggests that a number of treatments with corticosteroids over a number of years affects the risk of developing osteoporosis. Clearly, this cannot be ruled out by this study, which claims to have found a link ‘independent of medications’.
Therefore, the conclusions made by Sin et al. (2002) go far beyond what the data can show, and, as such, these unsupported conclusions – especially given the weight of evidence to the contrary – should be ignored. However, given that the data about BMI and age appears to be sound, the conclusions drawn in these areas should not be ignored, but equally cannot be extrapolated and applied to the population as a whole without further studies being conducted on other sectors of the population.
Given that both of these studies appear to have quite major flaws, this creates difficulty in knowing whether or not corticosteroids are a cause of osteoporosis in COPD patients, and it is clear that more research needs to be done in this area in order to make any firm conclusions.
Discussion and Conclusions
Through completing this SSC, it has become clear to me that there is little definitive research into the links between COPD and osteoporosis. This is, perhaps, surprising, given that osteoporosis as a disease greatly increases morbidity in patients. However, given that COPD has only started to be recognised as a condition in its own right relatively recently (Barnes et al, 2002), and given therefore that treatment regimens are still being developed, it is understandable that little research has yet been done into the affect of COPD on other diseases.
Looking over the literature review and the critical appraisal together, it is clear that the hypothesis proposed by Dubois et al. (2003), which to me appeared to be the most promising, does not have enough real evidence to support any firm conclusions. Clearly, more work needs to be done to either prove or disprove this hypothesis.
As with most conditions in medicine, when a link is finally established, it is likely to be formed from a number of different factors, and to attempt to find a link simply between drug treatments and COPD is probably over-simplifying the reality. The ideas presented by Biskobing (2002) probably have much merit, but clearly research needs to be done to find which of the factors she suggests affect osteoporosis are the most important, so that these can be either treated or avoided during treatment.
Without knowing the most important factors, it is difficult to make recommendations as to whether screening all COPD patients for osteoporosis is the correct course of action to take. To screen all patients when only those with a certain – as yet unknown – risk factor develop osteoporosis would not be a sensible way of using resources, but without the luxury of knowing what this factor is, this is not an option. However, if we consider the substantial increase in morbidity afforded by developing osteoporosis, as well as the stress and distress this confers on patients, in addition to the relative ease of monitoring and acceptability of this to the patient, it would seem prudent (in an ideal world) to monitor all COPD patients until further research is done to confirm the specific risk factors. Of course, with limited resources, it would be necessary to further assess whether the cost of such monitoring would be worth bearing considering the financial support that would have to be removed from elsewhere, but taking into account the factors outlined, I believe that monitoring such patients would, indeed, be an appropriate use of resources.
I feel that this study has provided a valuable lesson to me as a developing medical student, as it has highlighted the fact that clinicians and researchers do not have all of the answers. I posed a challenging clinical question, and found that no definitive solution can be offered at present. This could be a difficult concept to explain to a patient in a different scenario, if they had a particular clinical condition and the best treatment were not yet known, for example. This could be made particularly challenging if the patient had found some anecdotal evidence that a particular treatment was best, and yet the balance of evidence is tipping in the direction of a different treatment. Such a situation would require delicate handling, and would be a true test of effective communication skills.
During this study, I have learned much about the science of the interactions between glucocorticoids and osteoporosis, as well as about osteoporosis and COPD as diseases. I have also learned about being careful to make sure that the claims of a paper do not exceed the evidence actually presented.
Overall, despite being unable to find a conclusive answer to the original question I set myself, I feel that completing this SSC has provided an extremely valuable learning experience, which has allowed me to gain much that will help me during my future medical career.
Bibliography
Barnes P, Drazen J, Rennard S and Thomson N (2002) Asthma and COPD: Basic Mechanisms and Clinical Management London: Elsevier Science » Buy Now
Biskobing DM (2002) COPD and Osteoporosis Chest 121(2):609-620
Crookston JH (2002) The Crookston Collection [online]
Available from http://www.thecrookstoncollection.com [accessed 2nd April 2005]
Dubois EF, Röder E, Dekhuijzen PNR, Zwinderman AE, and Schweitzer DH (2002) Dual Energy X-Ray Absorptiometry Outcomes in Male COPD Patients After Treatment With Different Glucocorticoid Regimens Chest 121:1456-1463
Karadag F, Cildag O, Yurekli Y, and Gurgey O (2003) Should COPD patients be routinely evaluated for bone mineral density? Journal of Bone and Mineral Metabolism 21:242-246
Kowalchuk RM, and Dalinka MK (1998) The Radiologic Assessment of Osteoporosis University of Pennsylvania Orthopaedic Journal 11:67-72
Melton LJ, Patel A, Achenbach SJ, Oberg AL, and Yunginger JW (2004) Long-term fracture risk following adult-onset asthma: a population-based study Osteoporosis International 15:311-316
National Institute of Health (2003) The Low-Down on Osteoporosis: What We know and What We Don’t [online]
Available from http://www.nih.gov/news/WordonHealth/dec2003/osteo.htm [accessed 5th April 2005]
Sin DD, Man JP, and Man SFP (2003) The Risk of Osteoporosis in Caucasian Men and Women with Obstructive Airway Disease The American Journal of Medicine 114:10-14
Walsh LJ, Lewis SA, Wong CA, Cooper S, Oborne J, Cawte SA, Harrison T, Green DJ, Pringle M, Hubbard R, and Tattersfield AE (2002) The Impact of Oral Corticosteroid Use on Bone Mineral Density and Vertebral Fracture The American Journal of Respiratory and Critical Care Medicine 166:691-695