Fish oils and cardiovascular disease
This assignment consists of a critical appraisal of the evidence for fish oils and their effects on the cardiovascular system. A full bibliography of sources is provided at the end. Click on figures and diagrams to enlarge them.
Please remember that this is merely a medical school assignment, and does not constitute medical advice.
Critical Appraisal
It has been recognised for many years that the Greenland Inuit population exhibits a lower death rate from acute myocardial infarction than the population of Denmark, despite there being little difference in blood cholesterol levels between the populations. It is now known that this is due to the populations’ differing diets, and specifically the amount of omega-3 fatty acid consumed. (Holub, 2002)
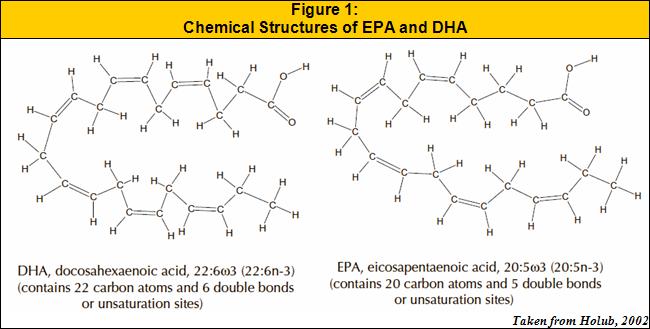
Omega-3 fatty acids are long-chain polyunsaturated fatty acids. The main omega-3 fatty acids found in fish oils are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). These two particular fatty acids exhibit a strong negative correlation between levels in the blood and cardiovascular disease events.
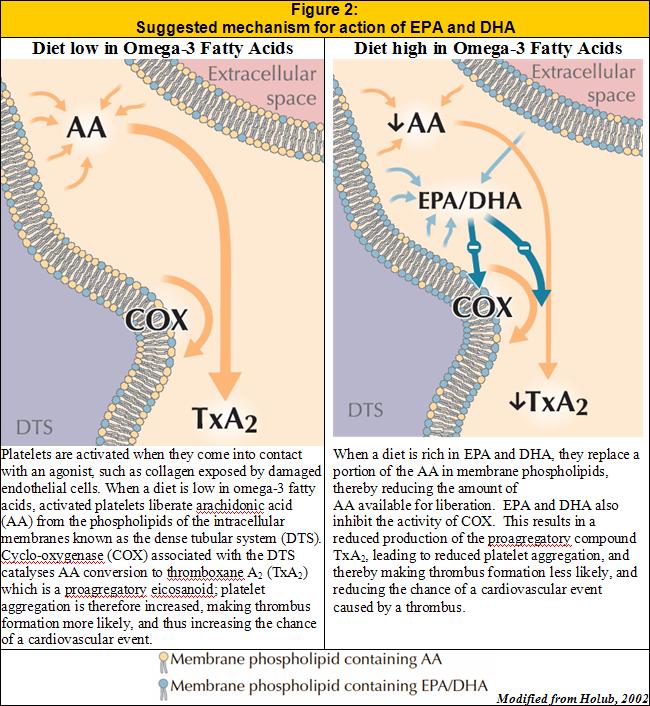
In his review, Holub describes a mechanism by which increased dietary intake of EPA and DHA may reduce the number of cardiovascular events. He suggests these fatty acids induce an anti-thrombogenic state by reducing the amount of platelet aggregation in the blood:
Holub also explains that other important mechanisms by which EPA and DHA reduce the number of cardiovascular incidents include their apparent antiarrythmic, blood lipid lowering and blood viscosity lowering effects. It is this wide range of effects which makes fish oils a particularly effective treatment: Where most drugs act by only one mechanism, fish oils exhibit a multi-faceted approach to preventing cardiovascular disease.
Holub concludes that most people should eat more fish, consuming one portion of fatty fish per day, or alternatively taking a fish oil supplement, since this would increase the intake of EPA and DHA to around 900mg per day – levels that have been shown to be beneficial to patients.
The GISSI-Prevenzione trial (GISSI-Prevenzione Investigators, 1999) examined the effects of dietary supplementation with omega-3 fatty acids and vitamin E following a myocardial infarction. The investigators enrolled patients who had suffered myocardial infarctions within the past three months. They chose not to specify age limits, and chose only those patients who had no unfavourable short-term outlooks. They randomly assigned each of these patients either supplementation with vitamin E, omega-3 fatty acids, both, or no supplementation.
Over a series of follow-up visits, the investigators found a significant decrease in the rates of death, non-fatal myocardial infarction and stoke in those patients who were given omega-3 supplements, whether alone or combined with vitamin E. The dose given to the patients daily was 1000mg, which is clearly more than the level that Holub defines as “beneficial”, and so it would appear that their findings fit together.
The GISSI trial does have a few problems: It is not noted whether those patients not given omega-3 supplements ate fish, thereby receiving omega-3 anyway, and also that the trial was not blind, and so preferential treatment may have been given to some groups by medical staff. Despite this, it is clear that this trial adds further weight to the argument that omega-3 fatty acids are beneficial in cardiovascular disease.
The trial conducted by Siscovick et al. (2000) took all primary cardiac arrest cases aged between 25 and 74 attended by paramedics in Seattle and King County over an eight year period, and closely matched each subject with another from the population according to age and sex.
The researchers questioned each of their subjects on their intake of omega-3 fatty acids over the preceding month. Clearly, this is not a terribly reliable way of obtaining this data, since it would not seem terribly likely that subjects would be able to remember the details of fish they had eaten for a whole month preceding the interview. In order to try and combat this problem, their partners were asked to try and help them to remember. The team also decided to assess the dietary intake indirectly by taking blood and analysing the fatty acid composition of the red blood cell membranes – a rather more accurate measure than trying to get subjects to recall their dietary habits.
The study found that an intake of one fatty fish meal per week was associated with a reduction of 50% in the risk of primary cardiac arrest. This is equivalent to under 200mg of omega-3 fatty acids per day, and yet a marked reduction in the number of events has been shown. Furthermore, the researchers found no evidence that higher intake than this increased protection. This is clearly at odds with the findings of the other studies discussed. I suspect that the reason behind this difference is at least in part due to the relatively poorer methods used by Siscovick et al. Despite their fairly poor methods, I chose this study as it attempted to retrospectively examine fish intake in the ‘real world’, rather than the highly standardised conditions of most studies. Despite the disagreements, this study clearly agrees with the others in that regular consumption of omega-3 fatty acids reduces the number of cardiovascular events.
In contrast to the less accurate methods employed by Siscovick et al. (2000), I have also chosen to examine a very highly controlled trial conducted by von Schacky et al. (1999). In this study, the researchers took 223 patients with angiographically proven coronary artery disease, and treated them for two years with either fish oil concentrate or a placebo. After two years, the patients had another standardised angiogram, which was then compared by a panel of experts to the original. The aim of the study was to discover whether the omega-3 fatty acids would have any beneficial effect on coronary atherosclerosis.
The study found that in the placebo group, 85% of the group had some degree of progression of the disease, compared with 71% in the fish-oil group. Also, whilst only 14% of the placebo group saw any regression in the disease, regression was seen in 29% of the fish-oil group.
After careful statistical analysis of these figures, taking into account the small study size, the researchers conclude that intake of the fish oils “modestly” mitigates the course of coronary atherosclerosis. However, given that the researchers found no negative side-effects of the treatment it would appear that, even if it mitigates the course of the disease only “modestly”, it is worthy of consideration.
The final article I have chosen to discuss is an American Heart Association Scientific Statement (Kris-Etherton et al., 2002), giving their opinions and advice on treatment and prevention of cardiovascular disease with fish and fish oils. This review is the only one of the articles that specifically deals with the safety of long-term consumption of fish and omega-3 fatty acid supplements, an issue recently highlighted in the media. The AHA claim that well-prepared omega-3 supplements contain virtually no environmental contaminants, but those less well prepared may contain appreciable amounts. This is unfortunate, since I think that most people will try and find the cheapest supplements available, and so potentially be taking harmful chemicals along with the omega-3 fatty acids. The AHA should, perhaps, have recommended tighter controls on production of these supplements in order to ensure that only high quality ones are produced.
Despite the evidence of the benefits of fish consumption, the AHA are rather restrictive in their recommendation of fish consumption, recommending instead that “consumers need to be aware of both the benefits and risks of fish consumption for their particular stage of life”. The reasoning behind this rather reserved advice is that the AHA found that some species of fish contain significant levels of methylmercury, polychlorinated biphenyls (PCBs), dioxins and other environmental contaminants, meaning that pregnant women, children and lactating women who are at low risk for CHD anyway may do more harm than good by eating a lot of fish.
Therefore, whilst all of the articles I have discussed conclude that omega-3 fatty acids found in fish oils are particularly beneficial to patients at high risk of cardiovascular disease, it is, perhaps, unwise to issue blanket recommendations for everybody to try and eat at least one fishy meal per day, as recommended by several of the articles, since the adverse effects of eating the fish may outweigh the benefits. It may be more prudent to advise those at particular risk from cardiovascular disease to increase their fish consumption slightly, and to use well-prepared fish oil supplements to help reduce their risk of cardiovascular disease.
Bibliography
GISSI-Prevenzione Investigators (1999), Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. The Lancet, 354(9177):447-455
Holub, B.J. (2002), Clinical Nutrition: 4. Omega-3 fatty acids in cardiovascular care. Canadian Medical Association Journal, 166(5):608-615
Kris-Etherton, P.M., Harris, W.S. and Appel, L.J. (2002), Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease. Circulation, 106(21):2747-2757
Siscovick, D.S., Raghunathan, T.E., King, I., Weinmann, S., Bovbjerg, V.E., Kushi, L., Cobb, L.A., Copass, M.K., Psaty, B.M., Lemaitre, R., Retzlaff, B. and Knopp, R.H. (2000), Dietary intake of long-chain n-3 polyunsaturated fatty acids and the risk of primary cardiac arrest. The American Journal of Clinical Nutrition, 71(1):208-212
von Schacky, C., Angerer, P., Kothny, W., Theisen, K. and Mudra, H. (1999), The Effect of Dietary ω-3 Fatty Acids on Coronary Atherosclerosis. Annals of Internal Medicine, 130(7):554-562